Aphy Mputu
Independent researcher, Luxembourg
https://orcid.org/0009-0001-2677-9142
Status: preprint, open to discussion and academic collaboration; originally written in French, this is the author’s English version.
Version: 1.0 (June 2026).
Convention: citations follow the (Author, year) format; full references are listed at the end.
License: the conceptual contributions are released under a CC BY 4.0 license (see Declarations).
DOI: https://doi.org/10.5281/zenodo.20646691
Abstract
Burnout has no agreed definition. But one fact is beyond dispute: at some point, people collapse, exhausted. The phase that leads up to that collapse goes unrecognized while you are in it. Its signs are there, often felt, but rarely read for what they warn of. Stage models already describe how symptoms worsen and follow one another. This paper maps the configuration of that prodromal phase: the arrangement behind both its slide toward collapse and its illegibility, for the person living it and for those around them. You cannot take stock of a territory you do not recognize, so naming this illegibility comes first. If the crossing turns out to be recognizable ahead of time, a window for orientation opens. Its clinical value still has to be tested.
The paper names this territory the gray zone (T0, the switch that opens it; T1, the collapse that closes it), and the mode that occupies it Survival Functioning: holding up what must be held even when resources have run short, by drawing ever harder on their reserves.
It proposes an entry marker (recovery no longer restores) and an exploratory criterion for locating the crossing. Several mechanisms account for the failure to see, each enough on its own; their convergence is not required.
A compensatory loop sets in and sustains itself, drawing down resources all the way to collapse. Illegibility is treated as a configurational property, still to be tested: it comes from how the background, the demanding context, and the mode are arranged, not from any trait of the person or the organization.
The method is an abductive inquiry (Haig, 2005): it starts with the observable collapse and works backward to what led to it. It is written up as a theory synthesis paper (Jaakkola, 2020). The cases it draws on were all selected because they ended in collapse, so burnout serves here as an anchoring case, not the only way the gray zone can end. The shape of the trajectory is offered as transferable. That, too, has to be tested. Two testable propositions are put forward for empirical work. The first is whether practitioners trained on the map can spot the gray zone better than they do today; the second is whether that recognition holds up from one judge to another. Other lines of research go with them: turning the marker into a short, repeatable measure; and tracking, over time, whether more time in Survival Functioning brings a heavier toll after the collapse. This last one is a prediction you can test on its own, apart from the definition.
Keywords: gray zone, Survival Functioning, burnout, prodromal phase, configurational illegibility, entry marker, abductive inquiry, theory synthesis paper.
Terminological convention: the notions this paper introduces appear in bold at first mention (gray zone, Survival Functioning, entry marker, and so on). Established constructs borrowed from the literature are set in italics (goal shielding, surface acting, overcommitment, allostatic load, and so on). Among them, mislabeling and discounting are existing constructs used here in the specific configurational sense set out in §7.
Author’s positioning
This paper is a practitioner’s work. In April 2021, after five years at a tech company, I was placed on sick leave for severe burnout. A certified coach since 2019, I had not seen the collapse coming. The doctor prescribed a first ten-day leave and put it plainly: “to see whether rest works.” That sentence showed me rest could fail to work; the ten days confirmed it. The word he had used, burnout, did not match what I felt: I did not feel ill. Without words, no handle. That missing handle set the work going. I carried it on supporting others, first inside companies and then in my coaching practice.
First, to put it into words: to describe the experience in everyday language, until the phrase gray zone emerged for the phase before the collapse, and then to support others and write for a general readership. Looking for firmer anchors revealed the obstacle: the burnout field had little structure built around the prodromal phase as an object in its own right, while the conceptual pieces it needed already existed, scattered across separate fields. That scattering is what calls for integration rather than a new theory, and what led to this paper.
This integrative work is a theory synthesis paper (Jaakkola, 2020): a framework that ties existing theoretical elements, each documented in its own field, to phenomenological names of its own, in order to grasp a phenomenon and make it a named object. It is rooted in reflective, engaged practice (Schön, 1983; Van de Ven, 2007) and proceeds by abduction: starting from the observable phenomenon, proposing a representation of it, then linking that to existing theories before any empirical test (Haig, 2005). From Theory Construction Methodology (Borsboom et al., 2021), it takes only the opening move, from phenomenon to prototheory, without carrying out the formalization, which is left to later work.
This status sets the criteria for judging it. A theory synthesis paper is not judged by the immediate falsifiability of its statements: it is not a closed theory putting forward predictions to be refuted. It is judged by what it does: holding together pieces that were scattered, cutting its object at the right joint, opening paths others can take up (Jaakkola, 2020). That does not place it beyond testing. A map is only useful if it stays faithful to the territory it represents: what the propositions in §9 put to the test is therefore the recognizability of the territory it points to, not the truth of the map. Offered on those terms, the map is used modularly: it notes bridges to constructs from separate domains, and each construct appears as an anchor, kept for the role it plays in the map, not for its place in the literature. Readers take from it what serves them: a landmark, a mechanism of illegibility, a background concept, or something else.
This paper isolates one thing: the theoretical characterization of the prodromal phase. By contrast, the practitioner framework behind some of the elements brought together here (the MABI, named in the transparency declarations) offers tools for support, training, and burnout prevention, and draws on intervention protocols specific to the author’s practice; that support work, with its progressions and contraindications, belongs to a separate practitioner’s manual and falls outside the scope. Nor does the paper settle the diagnostic distinction between burnout and the neighboring clinical entities, with which it shares observable markers such as anhedonia. The gray zone is not a nosological entity competing with others: it does not answer the question “which disorder is this?” but characterizes a way of functioning as it is lived through. The same person may later receive a diagnosis from a health professional (depression, full-blown burnout) without that overturning the map of what they were going through before; telling them apart is the work of validated instruments, which the map does not replace (§10).
This situated stance is both what made the paper possible and its main limit. What made it possible: the author has crossed the territory he describes and has supported people crossing it. The limit: work produced from this vantage point cannot rule out that what it points to reflects, in part, the configurations specific to the setting it came from. The propositions put forward in §9, with their explicit rejection conditions, answer this limit methodologically: they expose the mapping to an independent test.
1. Introduction
Every year, people buckle under burnout. Not just tired, drained. Collapsed. Unable, overnight, to do what they were doing the day before. In my practice, the same phrase comes back again and again: “I didn’t see it coming.”
And yet the signs were there, beforehand, many of them, ordinary, each explainable on its own. The workload rose, pressure became routine, stress settled in, coffee went from two cups a day to six, or more, with no one paying it much attention. The weekend hobby had been “postponed” for weeks, first one, then two, then they stopped counting. Sleep restores less and less: the person wakes up as tired as when they went to bed, and blames the mattress, the stress, the season. A knot in the stomach shows up on Sunday evening, at the thought of going back to work the next day. It was not there six months earlier, but “you make do,” because it set in gradually. The partner says: “you’ve changed.” The person does not see what they mean. And one phrase among others that comes back without fail: “I just need a vacation.”
None of these signs, taken on its own, was alarming. Each had a reasonable explanation. The person felt them without really grasping them; those around them saw some without being able to connect them. Both missed the same phenomenon, for different reasons (which we will come to later). And if both miss it, it is because these signs are not of the same kind: some come from the body, others from thought, others again from relationships. That is why they do not come together on their own: connecting them means crossing fields we usually keep apart.
The burnout this trajectory converges toward is itself a paradoxical object: institutionally, legally, and clinically recognized, yet without a consensus definition or a stable nosological category. A 2018 systematic review in JAMA counted 142 distinct definitions and a prevalence among physicians ranging from 0 to 80.5% depending on the definition used (Rotenstein et al., 2018). The ICD-11 listed it in 2019 (in force from 2022) under the code QD85, in the chapter on factors influencing health status, as a work-related phenomenon (an “occupational phenomenon”), not classified as a medical condition (World Health Organization [WHO], 2019). The International Labour Organization (ILO), in its global report on the psychosocial working environment (April 2026), documents the scale of psychosocial risks at work, where exposure is typically sustained over time (ILO, 2026).
Clinical practice identifies it without the ambiguity the definition carries: doctors, occupational health services, and specialist clinicians know how to spot it, not from a questionnaire score but from a body of converging evidence drawing on clinical signs, working conditions, and individual susceptibility factors (Haute Autorité de Santé [HAS], 2017). In France, more than 1,800 work-related mental health conditions were recognized in 2024 through the supplementary route (Assurance Maladie – Risques professionnels, 2025). Across Europe, burnout is recognized as an occupational disease only in some EU member states, with wide variation in how it is recognized and compensated (Lastovkova et al., 2018).
The Burnout Assessment Tool (BAT; Schaufeli et al., 2020) provides an instrument-based operationalization of it, and cutoffs have since been established on three European samples (Schaufeli et al., 2023). In 2025 the field is going through a debate about its conceptual foundations. The positions in it, including the proposal to replace burnout with a category of occupational depression (Bianchi & Schonfeld, 2025), lie outside this paper’s scope. At the same time, the field is calling for a renewal of its theoretical frameworks to account for complex mechanisms (Demerouti & Bakker, 2025). This paper is about what happens before this object, not about redefining it or settling its diagnostic boundaries.
This is where the questions it addresses come from. When did these signs appear? How did they intensify without raising the alarm? Why were they not read for what they were signaling? Why in some people and not others? The angle dictates the method: an abductive inquiry that starts from the collapse (the observable fact) and works back toward what led to it. The approach is therefore retrospective: once the collapse has happened, it reconstructs what came before. Still, whether these markers truly came first, as opposed to being projected backward after the fact, is an empirical question: the literature recognizes early signs of burnout, documented among health professionals (Karakolias, 2025), and a prospective protocol (§9) would establish their timing.
The territory that comes into view in this movement, where these signs arise and intensify without being read, is what this paper calls the gray zone.
The fact that signs precede the collapse is not new: models have long described how burnout progresses through ordered stages (Freudenberger, 1974; Golembiewski & Munzenrider, 1988; Parker & Russo, 2025). This paper focuses on that period. It reconstructs its map, with its boundaries, its mechanisms, its configuration.
In this phase the person is still holding up and does not see themselves as ill, so they seek little or no care for it; the “I just need a vacation” line is one example. Validated instruments therefore barely come into play yet: they measure a state once the person reaches care, most often at the collapse or after. The phase before it can then only be observed on trajectories that have already run their course (§9).
The visible sequence, the collapse and then full-blown burnout, is the one everyone recognizes; this work is about what comes before it. We begin with a case, Sarah, who will be our touchstone in what follows.
2. The interview with Sarah
Sarah is a composite case, built from recurring patterns observed in companies and then in coaching practice. The method, standard in the social sciences and in clinical research (Willis, 2019; McElhinney & Kennedy, 2022), shows a typical configuration through a lived account. We follow that account for what it makes visible: elements that are often familiar from the literature, not always linked to burnout, and that we then take up one by one. Sarah matches no real person, no biographical detail points to an identifiable clinical case, and no personal data is processed. This chapter sets down the material of the interview, staying close to her own words, up to the pivot question it closes on, which §4 will take up as the entry marker. The analysis begins in the next chapter.
Sarah has been on sick leave for three weeks. She is no better.
Before this leave, Sarah was what every manager dreams of having on their team. Seven years at the same company, three promotions, spotless reviews. She ran her own area, carried the cross-functional projects she was handed, and still found time to train the new hires.
When I meet her, she is completely lost. She does not understand what is happening to her, and she does not recognize the person she has become, the one who can no longer get up in the morning, who cries for no reason. Nothing makes sense anymore. Her anxiety is intense, all the time. She is on leave, but her system is not.
I have to find a solution fast, she tells me. People are counting on me.
She feels guilty: toward her colleagues, her manager, her family. Her worry is not only for herself; it is for the people she feels she is letting down. Sarah built her life, her identity, around this: being the one others can count on. And now that she can no longer be that, she is no one anymore, or so it feels to her.
My therapist asked me: “What could you do for yourself, something you’d enjoy?” And it was crystal clear: “NOTHING!”
This is not discouragement, and it is not a passing low. It is an inability to feel pleasure in what used to give it. Sarah loved gardening, long Sunday morning walks in the forest, and cooking for her friends. These activities have not vanished from her memory. They have vanished from her drive. When she tells herself: “I should go out to the garden,” nothing stirs.
Before her collapse, Sarah speaks of a hard stretch.
The months before my sick leave were really stressful. Two colleagues quit one right after the other. But I was okay… I had to keep holding on anyway… The coffee helped… a bit too much, maybe…
The anxiety was already there, months before, but not as strong… The stress too, trouble concentrating… More than once, I wanted to drop it all… I was in survival mode…
And then Sarah catches herself:
And yet I did everything you’re supposed to do to be well. Yoga, anti-inflammatory food, cut out gluten, got a coach, saw a physio for tension that won’t ease anymore. I even saw a naturopath. But it didn’t work. I held on, but I don’t know why, I just can’t anymore.
Before she collapsed, Sarah held on for a long time under intense stress, almost a year. She went to work, met her deadlines, smiled in meetings, answered “fine” when asked, and meant it. From the outside, nothing showed. Her manager found her “as reliable as ever.” Her colleagues suspected nothing. Her partner saw she was tired, but who isn’t?
Her functioning held, at least on the surface. That was all that mattered. And because her functioning held, no one around her saw the collapse coming. What she did not see, what no one saw, was the cost of that functioning. The price her body paid every day to keep up this appearance of normalcy.
And I don’t understand why I still feel so tired, so awful…
Sarah reaches the end of what she can put into words. She has described her state: the anxiety, the helplessness, the absence of pleasure, the bewilderment. But there is so much she has not said, not because she is hiding it, but because she does not have the words.
Then I ask her a question: does your rest actually rest you?
Sarah is taken aback. No one has asked her this, not like this, not in these words. Her doctor asked how she was sleeping. Her coach asked whether she took breaks. Her psychologist asked whether she made time for herself. Her physio recommended exercises, and getting out for walks, in the forest if possible. The naturopath talked to her about nutrition. But no one had asked whether that rest produced anything: whether, in the end, she felt recharged.
After a long silence, she answers: “No.”
That “no” resonates. It opens something deeper.
I ask her: “Since when?”
She stays silent, then finally says: “I don’t know, it’s been a long time now…”
3. Markers of suffering, read backward
The interview with Sarah has set down dense material, a solid base of work that we can begin to analyze.
The first thing to note is the collapse itself. Overnight, Sarah found herself unable to return to work. And since that day, what she voices most often is distress, a constant suffering.
Full-blown burnout, the kind that sets in after the collapse, has known markers of suffering: exhaustion, stress, anxiety, trouble concentrating, sleep disturbances, among others (Maslach et al., 2001). We find several of them in Sarah’s account.
This suffering forms a broad cluster (§4); this chapter analyzes three of its signs. Two each have a distinct substrate: the stress that no longer comes down and the background anxiety that will not let go. The third, anhedonia, reads as an indicator of how far the crossing has already gone.
The stress that no longer comes down refers to an alarm system activation that no longer switches off, even at rest. It is not the acute response to a one-off threat, which rises and then falls back to baseline. It is a state of sustained activation in which the baseline itself has shifted upward, with a cumulative physiological cost on the regulatory systems: allostatic load in McEwen’s sense (1998), whose energy cost has since been modeled (Bobba-Alves et al., 2022).
The background anxiety that will not let go refers to a constant, free-floating apprehension that colors awareness without always attaching to a definite object. It rests on a different substrate: impaired prefrontal regulation under prolonged stress (Arnsten, 2009) and dysregulation of the hypothalamic-pituitary-adrenal axis (Fries et al., 2005). Stress and anxiety coexist in the crossing but operate on distinct substrates.
Anhedonia does not appear here as a marker of the same rank; it comes last and works as a depth indicator: it does not signal that the person is in the crossing, but how far along it already is. It refers to a withdrawal of pleasure where there used to be some: the capacity to feel pleasure remains; what goes out is the drive toward what once felt worth it. As resources get monopolized by holding the role together (Hockey, 1997; Shah et al., 2002), what used to be done for pleasure (a dinner with friends, a walk, a personal project) no longer produces the emotional resonance that gave it its value. What is described here is this withdrawal at the experiential level; tying it to a specific motivational substrate (the reward circuit) would belong to a separate literature and is not claimed at this stage. Reading this depth precisely is the practitioner’s work. This is what Sarah hints at when she says that nothing she tried in order to feel better worked: the practices were there, but their expected effect did not come. Anhedonia is also one of the markers burnout shares with neighboring clinical entities, including depression; reading it as a gauge of depth does not settle what is going on.
Read backward, these signs did not appear with the collapse, but before it. Sarah’s account reconstructs the stress that no longer came down, the anxiety and the anhedonia, and with them a broader cluster (fatigue, unrefreshing sleep, trouble concentrating, micro-collapses), as already present and growing well before her sick leave. This observation can only be made after the collapse; the signs themselves were present during the crossing. Recent literature recognizes such early signs of burnout (Karakolias, 2025), which supports this reading without proving it; exactly how far back they go remains an empirical question that §9 puts to the test.
One question remains: in what mode was Sarah functioning, for this suffering to set in and grow?
4. The gray zone
Sarah’s suffering emerged under conditions she described. She speaks of a hard stretch: two colleagues quit one right after the other, the workload rose, and “I had to keep holding on anyway.” The coffee “helped… a bit too much, maybe.” From the outside, her functioning held, at least on the surface. That was all that mattered. These elements say a great deal about the mode Sarah held, month after month, and out of which her suffering emerged.
The crossing that follows can be described in four movements knotted together (a visible front that holds, a compensatory loop that sets in, a rest that no longer rests, a suffering that unfolds across several registers) before the exit boundary is crossed (the dynamic is summarized in Figure 1).
Such a mode sets in within a particular context. On one side, intense pressure over a long period; on the other, fatigue that builds up. Once it has set in, this fatigue reaches a threshold beyond which the person can no longer function at the same level across everything they do. Their attention then narrows to what matters, while what is secondary is quietly let go: non-essential tasks, leisure, enough sleep.
This narrowing is not a quiet decline of “normal” functioning: it is the setting-in of another mode, the visible front. What the person holds first is what shows from the outside: what the manager notices, the deadlines, the meetings that count. What gives way is the rest: their own needs, what those close to them sense without being able to name.
But functioning while resources run dry has a cost: the boss’s email that asked for two minutes now asks for thirty, every sentence reread, weighed; the meeting where each contribution counts becomes an inner expense out of all proportion; tasks that were easy can take hours. This added cost comes from focusing resources on what must be held: compensatory control (Hockey, 1997) and goal shielding (Shah et al., 2002). This mode plays out as a whole visible front: the set of behaviors by which the person holds what shows. Several literatures have named fragments of it: impression management (Goffman, 1959) for the social part; surface acting (Hochschild, 1983), displaying an emotion one does not feel, for the affective part; overachieving (Salmela-Aro et al., 2019), performance kept up at the cost of health, for the output part, where strong engagement and strong burnout coexist. It is distinct from functional presenteeism (Karanika-Murray & Biron, 2020): in their four-cell typology, the maintenance described here occupies the cell where performance holds at the expense of health, not the adaptive cell where one works while unwell without making one’s condition worse.
Each of these literatures names a specific behavior, confined to the professional stage, that the person knows and manages. The visible front is broader: it is a mode, not an isolated behavior. It holds up everything visible, not just one facet; it spills beyond work (the grandmother in §6 has no one to convince); it is paid for out of vital reserves; and the gap it covers gradually stops being known (§7). Above all: these neighboring behaviors, the person knows; the visible front, they end up no longer seeing.
A compensatory loop sets in to make this maintenance possible. To hold up while resources run dry, the person draws on active compensations: coffee that doubles then triples, energy drinks, nights cut short to get ahead on work, supplements to keep going, weekends spent “catching up,” over-controlling the files, hypervigilance about anything that might go wrong, shortcuts on everything that is not critical. Each compensation works in the short term, at least at first, and comes from the same move: silencing the fatigue signal instead of answering it. It is precisely because it works that it repeats. But each repetition costs more energy, and that energy is already lacking; and by silencing the signal again and again, the person not only draws on low reserves, they undermine the rest that should rebuild them. The more fatigue rises, the less recovery works; the less recovery works, the more compensation intensifies; the more compensation intensifies, the more it draws on what is already short. The loop feeds itself, and each turn makes it heavier, until it feels like a steamroller. From the outside, the spiral is obvious: someone sleeping less, drinking too much coffee, working late, never switching off. Yet each compensation stays rational at the moment it is used, and that is what makes the loop hard to break. Why it is not seen, from the inside, as a spiral, §7 accounts for. It is a loss spiral in the sense of conservation of resources (Hobfoll, 1989), sustained by the failure of compensatory control (Hockey, 1997). Neighboring frameworks spell this out: the failure of self-regulation as the passage from acute stress to lasting burnout (Bakker & De Vries, 2021), or self-endangering work behavior, where extending working hours is paid for out of recovery (Dettmers et al., 2016).
Rest no longer rests. Well before the collapse, recovery begins to break down. What used to recharge no longer recharges: sleep, the weekend, vacations. This breakdown can be characterized in time: the rebound delay (the time the person needs to get back to their earlier state after a load) gradually lengthens. Two days were enough before; now it takes a week, then more. It is a behavioral observable, detectable without any prior theoretical grid (de Croon et al., 2003; Steptoe & Marmot, 2005; van Dam, 2021; Vandenabeele et al., 2025). Stress regulation is lost: the sustained activation no longer switches off, even at rest. The body stays in overdrive when the mind would like to catch its breath. The person keeps holding up, but no longer by choice: what they could no longer carry consciously, they now carry on autopilot. The pivot question, “does your rest actually rest you?”, finds its clinical anchor here, close to the criteria for exhaustion disorder (Socialstyrelsen, 2003).
This question, put to Sarah in §2, gives its shape to the entry marker of the gray zone (taken up again in §9 and §10). The marker is what a “no” signals: that recovery no longer restores. This landmark has a structural twin in research on symptom perception, where a trajectory likewise opens with a first event, the detection of a bodily change that starts the appraisal interval (Scott et al., 2013).
It does not stand on its own. It is read first alongside the convergence of the markers of suffering: the stress that no longer comes down, the background anxiety, the impaired recovery. And the rebound delay (its observable measure, whose lengthening can be seen) and the “impaired recovery” of the criterion point to the same deficit from different angles: with the marker, three operationalizations whose agreement remains to be established.
The pivot question provides orientation in real time and stays usable from the first meeting: the marker says you are in the territory, without dating the moment you entered it. That moment is T0 (§5), which can only be reconstructed after the collapse, for want of a prospective protocol. So the marker serves as an orientation point, and its psychometric operationalization, turning it into a short, repeatable instrument, remains an open research question (§9).
In this configuration, the suffering described in §3 sets in and widens. These signs, which we first saw downstream, after the collapse, are already there, and growing.
The four movements above can be summarized in an operational criterion, for research designs that call for an explicit threshold: five conditions that, when all present, help locate a person in the gray zone. A visible front still maintained (essential tasks held, the secondary scope dropped), active compensation, impaired recovery, established chronic stress, established chronic anxiety. None marks the crossing on its own; each can be observed elsewhere. It is their combination that makes the criterion.
The criterion leaves anhedonia aside: set out in §3 as a depth indicator, it runs through the gray zone but tells where the person is, not whether they are in it, and reading it finely is the practitioner’s work. Chronic stress, by contrast, holds a double status here: both one of the five observable conditions (the activation that no longer switches off) and the ground on which the self-sustaining mechanisms operate (§7).
It still needs calibrating, and it is not a clinical recognition grid: in practice, the practitioner reads the coherence of a pattern in the account, they do not list off conditions. §9 separates these two uses.
A word here for the reader who might recognize themselves in what precedes, or recognize someone they support. These markers describe a way of functioning; they do not make a diagnosis, and this map does not replace the opinion of a health professional, which should be sought without delay. For a practitioner who is not a clinician, recognizing the gray zone is a reason to orient the person toward such an opinion, not to take that role on.
The gray zone ends in the collapse: a dated event, where the visible front gives way. This is T1. The person then enters full-blown burnout, which lies outside the scope of this paper.
This chain brings us to a question: what pushes an apparently healthy person, whom nothing marks out as fragile, to tip into this trajectory and go all the way to collapse? What pushes them to want to hold on, rather than to say stop?
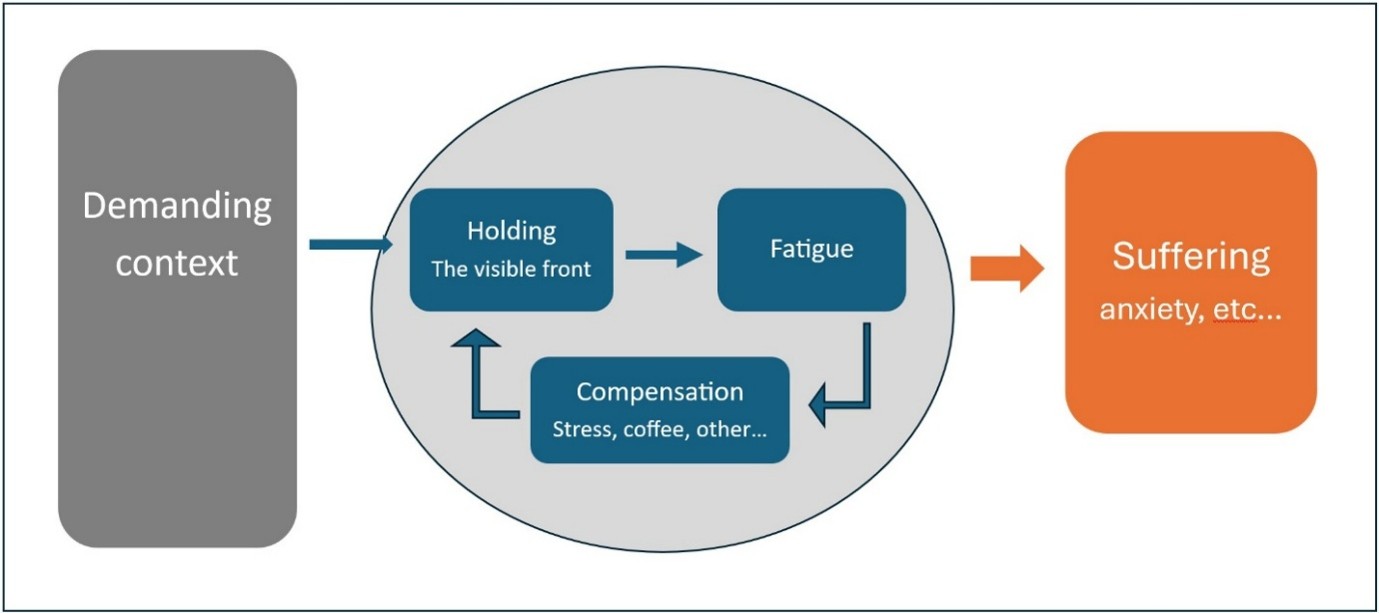
Figure 1. The compensatory dynamic of the gray zone: in a demanding context, the maintenance (“holding”) feeds the fatigue, which calls for compensation; this worsens the fatigue and lengthens the rebound delay, until the suffering sets in (anxiety, and so on).
5. Finding T0
Let us return to Sarah’s case. From the moment she was hired by the company, the level of demand was very high (company culture, pressure, tight deadlines, long days), but she adapted quickly and found her new baseline. To understand what tipped, and when, we have to go further back and tell two things apart: the background she brought and the context she met.
Preexisting background
Sarah built her identity around one thing: being the one others can count on. That is part of her preexisting background, what she carried long before she was hired by the company. Everyone has their own background, and it is irreducibly complex: personal history, values, beliefs, needs, fears, wounds, sensitivities, culture, habits, aspirations, sense of duty, discipline, shame, courage, need for recognition, physical vulnerabilities, rigidity, blind spots, and many other tangled elements, particular to each person. It is the personal ground in which a stressor may or may not take hold.
In other words, the preexisting background gathers the predispositions that push us to react in a particular way to a situation. For example, a latent allergy (the background) produces a reaction only on contact with the allergen (the context).
The background is not a list of independent factors: its components intertwine and modulate one another. This complexity, already hard to untangle with a clear head, becomes illegible for an exhausted person (§7). Its structure is stable; what varies is the activation and salience of its components under the effect of an event.
The background is not sufficient on its own, and it is not the only cause. Two people with comparable backgrounds may follow different trajectories depending on the context and the moment; but remove it from the configuration, and the configuration no longer holds together. It sets the threshold, the shape, and the speed of what follows, without being its engine: a non-redundant part of a configuration that, taken as a whole, produces the outcome. This is an INUS condition in Mackie’s sense (1965). The clinical literature has long distinguished predisposing factors (what the background brings, the configuration) from precipitating factors, the event that, in the timeline, triggers the switch (Spielman et al., 1987). The background belongs to the first; the triggering event, to the second. This paper borrows the distinction without adopting a stage grid: it does not sequence the trajectory, it maps a territory.
Demanding context
A position of responsibility, the life of a top athlete, the daily life of a parent of young children, preparing a doctorate: these situations have something in common. They call for a response equal to the demand, a sustained effort of adaptation, discipline, attention, diligence, a continuous mobilization of resources, sometimes sacrifices. This is what this paper calls a “demanding context.”
Where the two meet
But in some cases, a match occurs in the meeting between an element of a person’s preexisting background and a demanding context: a trait of the background resonates with what the environment values or demands. For example, a perfectionist working in an environment where precision and rigor are valued; an empathetic person in an environment that cares for the most vulnerable (for instance, care staff); a “performer” where performance is valued.
In burnout, certain components of the preexisting background recur: besides perfectionism and empathy, there are also the need for recognition and a strong identification with the role. The literature links them to the diathesis-stress model (Zubin & Spring, 1977) and to performance-based self-esteem (Hallsten et al., 2005).
This resonance is not universal, and it often appears as a stroke of luck rather than a problem.
Overcommitment
Faced with certain resonances, the person throws themselves in without counting the cost, becomes high performing, carries a great deal. Seen from outside, they are in their element; seen from inside, they find a meaning and an energy they may not have known before. It is here, in this investment that is not experienced as excessive, the overcommitment described by Siegrist (1996), that the trajectory begins.
Accumulation
What follows unfolds naturally but also silently. Accumulation first: the sustained investment loads fatigue and eats into resources, recovery still works but demands more and more discipline, and overdrive gradually becomes the norm.
Weakening
The hidden cost of performance builds up beneath the surface as a weakening: reserves run down, emotional stability erodes, and the tipping point, an invisible threshold, draws closer.
Back to Sarah’s case
For Sarah, it all started with an email she got on a Friday at 2 p.m.: “You have a presentation Monday at 10 with all the directors.” That week, she had been dreaming of her weekend, her walk in the forest, of resting. Instead, she froze for several minutes, collapsing inside, overwhelmed, not only by the email but by an “everything.” At that moment, all the paths that could have opened (refusing, delegating, asking for help, taking the weekend) are closed off by the felt threat and by the exhaustion that keeps her from even imagining them.
She rushed to the restroom, flushed so no one would hear, and burst into tears. After a moment, she pulls herself together. Her reaction is instinctive, a deep sense of having no choice: “Anything but that,” she tells herself.
When she came out of the restroom, she dried her tears, stopped by the kitchen for a double espresso, and went back to her desk, because “you have to hold on.” Not as a decision. The deliberative system has run dry. She does what she has always done: under intense stress and with resources spent, control of behavior tends to shift from deliberative circuits to habitual ones (Schwabe & Wolf, 2009), a mechanism whose scope has been qualified by recent preregistered replications (Smeets et al., 2023). The preexisting background supplies the program; stress runs the machine. That weekend, she worked Saturday and Sunday, on coffee and energy drinks. On Monday, her presentation went well. The directors were satisfied and her manager congratulated her. For the rest of that week, she even decided to keep up the momentum and catch up on what she was behind on. Above all, success, especially early on, is a diversion: the lift of the successful presentation, the praise, the feeling of being carried cover the fatigue rather than reveal it. Recovery is already eroded, though, and it would take more than a night of quality rest to make up for that weekend; but as long as the momentum carries her and she does not really stop, nothing signals it to her. She will only notice later, when the rest she finally takes no longer rests her.
At that moment, Sarah does not yet see that she will not go back. In a single weekend, her walk in the forest was set aside and then forgotten. She does not see that her whole mode of functioning has just switched (as if by default, without a decision) onto what she feels is essential, at the expense of the rest. This is T0: the moment the mode changes, a discrete switch, not a fatigue threshold that would worsen by degrees. The two are not the same: the weakening described above is a gradient that brings the system closer to its tipping point, but T0 is the moment of crossing over itself, the entry into the mode that the gray zone then settles into for the long term. A clarification is needed about the status of this T0: it is a narrative landmark reconstructed after the collapse, not a threshold detectable in real time. Sarah’s account places it, in hindsight, at that Friday email; at the time, nothing marked it as a switch. Dating it presupposes the view from after. Its very discreteness (a clean switch rather than a gradual slide) remains to be tested prospectively: seen after the fact, it may have looked clean where it was perhaps gradual. Making it a threshold that a practitioner could date in a person mid-crossing would require a prospective protocol (§9), which this paper does not anticipate. What mode then takes over, and how it holds for weeks or months without the person or those around them recognizing it, is what the following chapters will examine.
6. How to name this change in mode of functioning?
To make this mode visible, let us take a new composite case deliberately set outside the professional sphere and outside burnout.
A sixty-year-old grandmother, in good shape for her age, agrees at short notice to look after her two grandchildren, aged four and one, for three days. It is unexpected and no one else is available. The first night is sleepless: the younger one vomited at regular intervals, and she had to clean up, soothe, start over.
In the morning, she gets up with difficulty. At her age, a sleepless night is not just fatigue: her head hurts, her body hurts, stress is at its peak, anxiety sets in, the exhaustion is a kind of suffering, and a cognitive fog has settled. As a result, she has set aside her morning routine and exercises, and she has forgotten to take her medication.
Despite all these difficulties, something stronger keeps her standing: staying the grandmother who can be counted on in an emergency.
The very idea of failing in her role, of not being up to it, of letting her family down when they need her most, is simply intolerable. She has no choice, she has to hold on: an identity threat (Petriglieri, 2011), felt on a somatic register before it is thought (Damasio, 1994; LeDoux, 1996). Her whole normal functioning has switched over to something else. On the surface, she makes breakfast, changes the baby, speaks gently to the older child. She goes on existing as a grandmother. The older child does not notice that their grandmother is any different, and the neighbors who pass her in the hallway see nothing out of the ordinary. She carries out the actions that hold the situation together, and she carries them out competently. But she is no longer quite there. Her own hunger, her own thirst, her need to lie down, her pains and other bodily signals, all of it is there, but pushed behind the urgency of holding on, out of reach.
What set in for her on the morning of the second day is not a strategy. Her functioning narrowed by itself, without her having to decide it: the assessment of what matters happens below reflection, where Lazarus (1991) locates pre-reflective appraisal. A lifetime’s experience as a mother and then a grandmother takes over from what metacognition no longer has the energy to arbitrate, and the right actions come on their own, through the automaticity that expertise installs (Logan, 1988). Functioning then shrinks to the circuits that cost the fewest resources, short sentences, familiar routines, well-worn automatisms: this shift toward the least costly is the one mental fatigue documents (Boksem & Tops, 2008). And metacognition itself, the capacity to ask “am I doing all right?”, is saturated by the urgency of holding on: the crying baby pulls attention back to what must be done in the next ten seconds, not to the state of a life, a meta-awareness overwhelmed in Schooler’s sense (2002).
This mode deserves a name. The closest everyday term is “survival mode,” an expression widely shared in support practice and in the clinic, without ever receiving a formalization of its own. The term calls for an adjustment. In survival mode in the strict biological sense, all functioning not essential to staying alive is suspended.
What we observe in the grandmother operates on the opposite principle. It is elements essential to her own survival that the grandmother sacrifices to keep up the appearance of functioning well: sleep, bodily warning signals, recovery, vital reserves. This mode spends survival instead of preserving it. And it is the mode of functioning as a whole that switches, with reserves already eaten into.
We will call it here Survival Functioning (SF). SF is the mode in which the person keeps holding up what must be held, at the cost of everything else, while their resources are already short. This mode organizes itself around a felt threat (for the grandmother, letting her family down), and the person directs their strength toward one thing only: maintaining the visible front. It is this direction that governs the rest: it decides what the person still processes.
This mode forms at the meeting of three conditions: a demanding context, a lack of resources, and an element of the preexisting background that makes the idea of not meeting expectations unbearable for the person.
For the grandmother, the context is the emergency care of the two grandchildren, with all the effort it demands. The lack of resources is tied to her age, her health problems, and in her preexisting background there is a value, family, reinforced by the belief that you have to be up to it when your family needs you.
The demanding context exhausts and weakens, the lack of resources prevents the ordinary response, the preexisting background forces one to hold on anyway.
These conditions can converge quickly or slowly: the grandmother enters it on the morning of the second day; other people enter it after months or years, depending on the configuration. Duration is not constitutive of SF. Convergence is.
In these conditions, holding on has a direct consequence: with resources already short, the person sustains themselves by sacrificing the superfluous first, then the necessary, until they draw on the reserves that were meant to protect their integrity. This is the cumulative cost of sustained adaptation, documented by allostatic load (McEwen, 1998; energy cost modeled by Bobba-Alves et al., 2022). It is the lack of resources that separates SF from a sustained effort, however intense, carried out with reserves intact.
This draw has an empirical corollary, distinct from the definition: it leaves an observable trace. An accelerated weakening of the whole system, fatigue that does not yield to rest, heightened vulnerability to infection, persistent somatic tension, this toll is not deduced from the concept, it is observed after the crossing, and can be put to the test independently. Even the grandmother, after three days, will not recover at once; she may need several weeks to recover. Duration sets the size of the cost, not its existence. And this relation is itself an empirical claim, testable on longitudinal traces. This is the prospective path that §9 sketches: comparing the duration of SF against the magnitude of the post-T1 toll.
The gray zone is what is observed when this mode settles in for the long term, in a configuration where the demand renews itself without easing. What characterizes it lies in the arrangement of its elements, not in any one of them taken alone: the background, the demanding context, and the mode count only through the way they hold together. It is this arrangement that this paper calls a configuration, and it is this that the adjective “configurational” points to: a property of the arrangement, which reduces neither to a trait of the person nor to a feature of the organization. Sarah’s crossing, set out in §2, is an instance of this lasting deployment: the same mode as in the grandmother, but in a configuration where the demand renews itself week after week, where the weakening deepens, where what must be held recharges itself through identity. The grandmother will come out on the morning of the fourth day, when someone comes to relieve her. Sarah had no relief: the draw continued, week after week, until her vital reserves were eaten into to the point where even holding up ceased to be possible. This is T1, the collapse. The T0-T1 distance measures how long the configuration let the draw last.
An image throws light on this mode: an autopilot that holds course (the right heading stays on display) but whose sensors no longer respond. The aircraft flies straight; the overheating, the dropping altitude, the fuel running out no longer reach the dashboard. In the same way, SF orients the maintenance of the visible front while the internal signals (fatigue, depleted reserves) stop being read.
All this time, no one read it, neither she nor those around her. This failure to see is the subject of the next chapter.
7. The mechanisms of illegibility of the gray zone
The mode described in the previous chapter, and the configuration that sets in with it, remain partly illegible: some signs are misread when they reach awareness, and sometimes not perceived at all.
Four mechanisms produce the illegibility of the gray zone, on distinct registers: attentional capture turns attention toward what must be held; allostatic recalibration erases the reference to an earlier state; mislabeling fixes an ill-fitting name on what breaks through; discounting downgrades the signals that name does not cover. None is peculiar to the gray zone, and none is pathological by nature: they are ordinary operations of human functioning, which serve elsewhere, and serve well. What enlists them here in the failure to see is their operation within the configuration of the crossing.
Attentional capture
We saw with the grandmother how attention concentrates, under resource constraint, on what must be held at all costs: the visible front. This is the first cognitive consequence of the shift into SF mode, an automatic movement that no voluntary effort corrects. Everything outside it slips out of the field for lack of salience: one’s own fatigue, bodily signals, the overall trajectory, questions about oneself still exist, but do not get the attentional processing that would make them visible. This is the competition of cues (Pennebaker, 1982): attention, of limited capacity, continually arbitrates between internal and external signals, and the more the outside absorbs it, the less the body makes itself heard. In the gray zone, the arbitration leans permanently toward what must be held, which the focusing of resources on the goal prolongs (compensatory control, Hockey, 1997; goal shielding, Shah et al., 2002).
Allostatic recalibration
The brain notices what changes and gets used to what lasts. A continuous noise ends up unheard, a piece of clothing no longer felt. The internal state follows the same rule. When activation stays high long enough, it stops being registered as a departure and becomes the norm against which everything else is judged. This is allostatic recalibration: not a failure, but this ordinary mechanism applied to a state that should have stayed temporary. When a signal breaks through (a heart pounding at night, a fatigue that will not let go, concentration that falters), it is not read as a departure, for lack of a before to relate it to; over time, the person no longer compares themselves to a version of themselves they cannot find again. This principle also operates on the body’s signals: interoceptive processing dulls under chronic stress, and the signals that would allow comparison are received less faithfully (Schulz & Vögele, 2015). A physiological side adds to this: the organism readjusts its set points to support this level, a stability achieved through change (allostasis; Sterling & Eyer, 1988), whose accumulated burden is the systemic cost (allostatic load; McEwen, 1998; empirical support on burnout: Bärtl et al., 2022). A comparable drift has been described elsewhere, notably in ecology under the name shifting baseline (Pauly, 1995; Soga & Gaston, 2024); the analogy is heuristic, not mechanistic. The gray zone sharpens the effect: caught up in the present of what they hold, the person no longer has the mental room to go back to a before. Allostatic load tells the cost of it, the shifting baseline gives the image of it. Recalibration removes the reference: without that bearing, the other signals can no longer be read as departures.
Mislabeling
Faced with a sensation that does not give its name, we rarely stay without an explanation: we grab the most available word. A dip in energy is “I slept badly”; a tension is “it has been a rough week.” In the gray zone, the word at hand is fatigue. This is mislabeling. The label is consistent with recent history (a project that dragged on, shortened nights, weekends spent catching up) and socially available: people talk easily about fatigue, not about a nameless systemic decline. But it calls for responses calibrated on fatigue (rest, discipline, yoga, supplements), structurally unsuited to a state that is no longer fatigue. And it is because they do not work that the conclusion “nothing works” sets in: the lay representation of illness has calibrated the response on the wrong label (Leventhal et al., 1980).
Once the label is in place, it locks. Motivated reasoning takes over: the information that would contradict it (the rest that no longer rests, the ten-day leave that changed nothing, the naturopath who did not shift the state) is absorbed as a sign that the strategy was not carried out hard enough, well enough, long enough. The conclusion precedes the analysis, because letting go of the fatigue label would mean letting go of the strategy that follows from it, and that strategy is, in the person’s experience, what they have left to do (Kunda, 1990). Mislabeling thus assembles two familiar drivers, the lay representation of illness and motivated reasoning; but it is the only one of the four to supply a content, an active name that prescribes an action and holds it on the wrong target.
Discounting
A teenager, eyes on his phone, is told to be at the station a few minutes early, because the train will not wait. “Yeah, fine, I got it.” He will miss his train. The information arrived, it was even acknowledged out loud, and it changed nothing. This is discounting, the term transactional analysis uses (Mellor & Schiff, 1975). The construct is clinical, drawn on here for its descriptive aptness, not as an established empirical result. The signal reaches awareness, sometimes gets an explicit acknowledgment, then the silent label “not important right now.” It is neither denial, where a defense rejects a threatening content, nor ignorance, where the content is missing: it is received, named, but defused. In the gray zone, what passes this way are the signals that do not serve what one holds: a fatigue that weighs, a night-time heartbeat, a remark from the partner. The grandmother gives it its form: she knows perfectly well, from a lifetime as a mother and then a grandmother, that you cannot hold on for days without sleep or real meals, and she would say so to anyone. This knowledge, she does not apply to herself: it is there, repeated a thousand times, but it does not reach her when it would help.
Other factors affecting the gray zone’s illegibility
These four mechanisms do not close the list; others widen the failure to see, alongside the first ones. You do not recognize a sign you have never learned to look at: not knowing what it means to wake as tired as you went to bed, you take it for ordinary (ignorance). The mind, already worn, is precisely the instrument you would need to assess yourself: concentration crumbles, working memory falters, and clear-sightedness about oneself erodes with the rest (early cognitive loss). When a lucid reading does arrive anyway, an inner instruction leaves it without follow-up: “you have to hold on,” “people are counting on me,” “I have no right to let go” (the locking beliefs). And one also holds on for a team, a family, a lineage one does not want to let down, without always naming what holds one back (unconscious loyalties).
Taken one by one, these mechanisms are not new: each rests on an established construct, from the competition of cues to discounting. The research on symptom perception, the closest to this, has long studied them (Scott et al., 2013; Whitaker et al., 2015), starting from a sign already noticed, whose interpretation and then recourse to care it follows. This paper is about a mode that maintains itself and masks its own cost, where the sign, often, does not even reach the status of a sign. What it adds is their configuration: the way the SF mode turns each of these mechanisms toward what must be held.
Each of these mechanisms can, on its own, be enough to produce the failure to see. Most often, several act together and reinforce one another, but this combination is not necessary, and the four are not the only ones. Neither the person going through this state nor those around them have a clear view of it.
8. The missing language
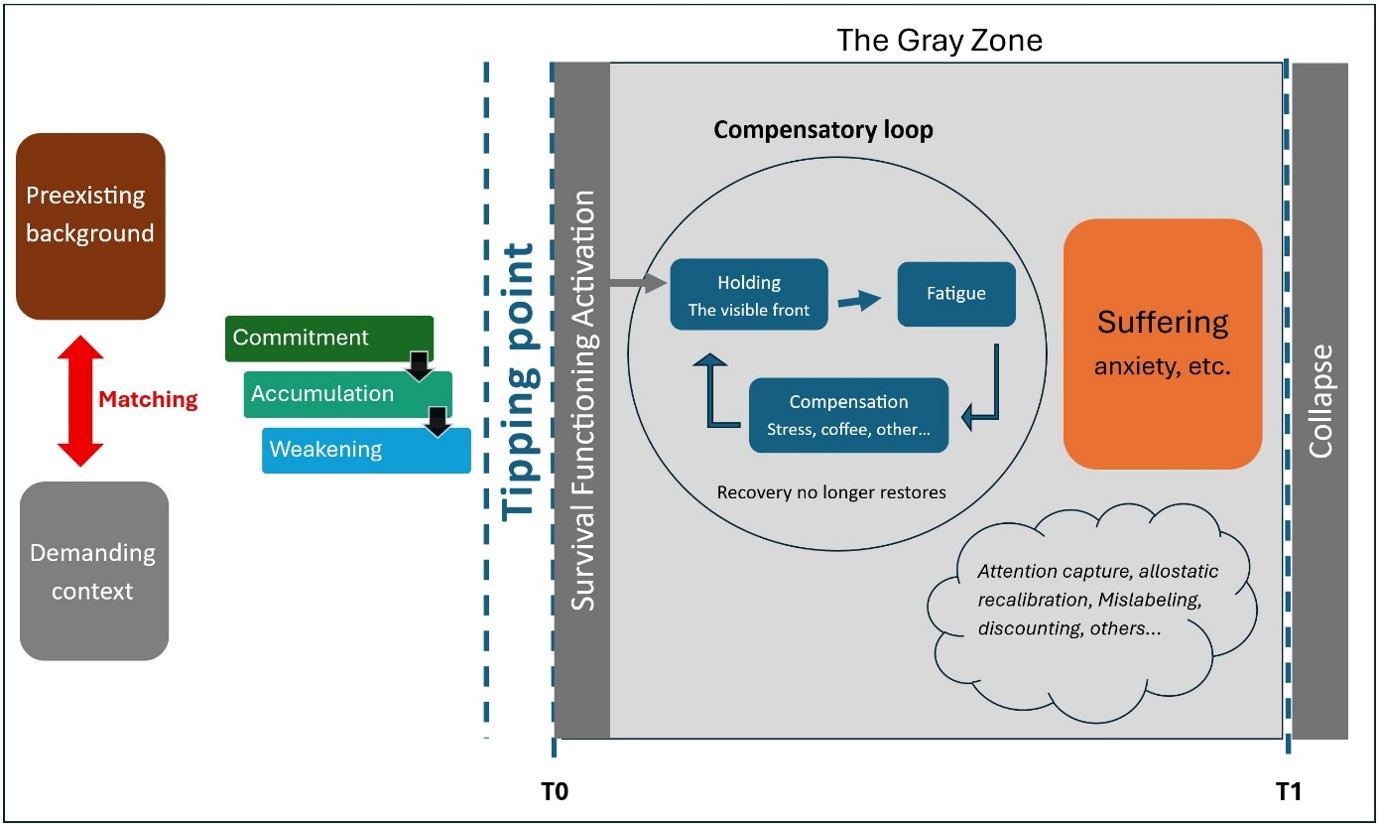
Figure 2. The complete map. A preexisting background meets a demanding context; at the tipping point (T0) the mode switches to Survival Functioning, which holds the visible front while recovery no longer restores, until the front gives way at the collapse (T1) and full-blown burnout. Throughout the crossing, four mechanisms keep the territory unread: attentional capture, allostatic recalibration, mislabeling, and discounting.
The whole territory can now be drawn as one map (Figure 2): the boundaries T0 and T1, the mode that crosses between them, and the four mechanisms that keep it unread. For a map to serve more than one person, it is not enough for it to be accurate: different practitioners have to be able to use it to point to the same thing. Three conditions state this. The first: that practitioners from different disciplines, each starting from their own practice, point to the same territory from the same markers (inter-disciplinary stability). The second: that a common set of materials be enough to train independent practitioners, without recognition depending on the talent of one or another (transmissibility). The third: that the person themselves, in the state they arrive in (exhausted, biased by mislabeling, hardly available to analyze themselves), can at least grasp its entry point (accessibility). These three properties are conceptual; §9 shows how to put them to the test, starting with the precondition they assume: that the map does distinguish its territory.
There is a precedent for this kind of move. In the 1990s, the prodromal phase of early psychosis was characterized by Yung and McGorry from retrospective clinical observation (Yung & McGorry, 1996), then operationalized in the following years by instruments that made its recognition shareable among psychiatrists, psychologists, and general practitioners. From there, the psychotic prodrome became an object of early intervention. Other shared tools in medicine work on a similar principle, few criteria, observable, with no disciplinary hierarchy, transmissible to trained practitioners: APGAR in neonatology, the Glasgow Coma Scale in emergency neurology, TNM staging in oncology (Apgar, 1953; Teasdale & Jennett, 1974; Brierley et al., 2017). The analogy bears on the form of these tools (few criteria, observable, transmissible), not on their status: their legitimacy rests on a body of empirical validation that the gray zone has not yet carried out. This precedent has its limit too: spotting a prodromal phase of psychosis does not guarantee that the person will ever tip over, and the risk there is the overmedicalization of people who are well. The mechanics differ here: the mode the gray zone points to has a cost in itself (rest no longer restores, the load builds up, §7), so that being in it is not being well. And this mode does not call for a medication: it calls for rest, but a rest that begins to rest again, which means lightening the load. Discriminance remains the issue, but it bears here on separation from an ordinary hard stretch, which §9 puts to the test.
Mental Health First Aid, an international public-facing program for recognizing mental health conditions, covers depression, anxiety, psychosis, addictions, and crisis situations such as suicide in its standard curriculum. In the standard international curriculum as described by the reference literature (Kitchener et al., 2015), it does not cover burnout. National adaptations may have addressed it, but the international core does not include it.
Another formalized clinical framework points to a neighboring state. In 2003, the Swedish Socialstyrelsen established a diagnosis of exhaustion disorder (ED), characterizing an established disorder of exhaustion, with criteria of duration, symptomatology, and loss of functioning (Socialstyrelsen, 2003; Glise et al., 2012). ED diagnoses an established, post-collapse state. The gray zone this paper maps lies upstream: the phase that precedes the moment such a diagnosis is made.
Sarah’s path at the start of the paper illustrates how persistent fatigue was received by five professionals: doctor, naturopath, psychologist, physio, coach. Each responded in their own grammar: rest, hydration, pleasure, the body, organization. The responses were coherent within each discipline. None bore on the territory Sarah was in. The observations that relate to it (the rest that no longer restores, the compensatory routines that grow longer, the tensions that no longer let go, the moments meant to give pleasure that no longer produce any, the dietary adjustments that no longer hold) were not connected to one another.
9. What the map offers up for testing
The characterization laid out so far (a prodromal territory, the boundaries T0 and T1, Survival Functioning, the compensatory loop, four mechanisms) is open to the test: testing it is the work of research. The two testable propositions described below are examples, neither exhaustive nor binding, of how a researcher might take hold of it. The first tests that the map distinguishes its territory; the second, that trained practitioners, from different disciplines where needed, agree on it. Accessibility is taken up further down, with the entry marker. They already come with their thresholds and their rejection conditions. The choice of what to test, and how, belongs to whoever takes it up. A recent review notes, moreover, that the timing and progression of the early signs of burnout remain poorly established (Karakolias, 2025).
First proposition: discriminance. A protocol could test whether practitioners trained in the mapping recognize the gray zone with a discriminance significantly higher than practitioners in their current practice. Trained here means: exposed in a standardized way to the mapping, having read the paper, with worked application cases. Discriminance means: higher sensitivity, specificity, and predictive value for the trained group. What remains is the standard to validate against, and that is the delicate point: a position in a prodromal trajectory cannot be fixed by expert consensus without circularity, since it is precisely that recognition which is at stake. The researcher’s choice proposed here is to anchor it on an observable, independent landmark (the actual crossing of T1), in a prospective design, the way the psychotic prodrome was validated against the transition that actually occurred rather than against a clinical judgment made a priori (§8). The rejection condition stays explicit: such a protocol would reject this proposition if trained practitioners were no better, upstream, than practitioners in their ordinary practice at picking out the trajectories that cross T1. The threshold for significant discrimination would be pre-specified in the protocol. But this proposition has a limit, and better to state it right away. Anchoring it on T1 means looking only at the people who collapsed. Those who crossed the same territory and got out another way, through a resignation or a project that ends, are not in the picture. So it can show that we spot the trajectories that go all the way better; it cannot say who, once in the territory, will collapse rather than leave by another door. This is the same selection limit that comes up later in this section.
Second proposition: transmissibility. A protocol could test whether practitioners trained in the mapping independently of one another reach sufficient inter-rater agreement on recognizing the territory. Sufficient means: a Cohen’s κ or a Krippendorff’s α above 0.60 (Cohen, 1960; Krippendorff, 2004), adjusted for the prevalence of the territory in the sample. The rejection condition is explicit: such a protocol would reject this proposition if inter-rater agreement among independently trained practitioners stayed below that threshold. The mapping would then not be transmissible in the claimed sense: it would remain individual know-how, not a shareable characterization. Transmissibility is the issue: what trained observers cannot agree on cannot anchor an academic object of its own.
These two propositions bear on the trained practitioner’s recognition of the territory: one tested against an independent observable landmark (the crossing of T1), the other against agreement among trained practitioners. They do not bear on the five-condition operational criterion (§4), which serves a different use: it is offered for research designs, and remains to be calibrated. A longitudinal study setting out to test the prodromal trajectory needs an explicit threshold. Clinical recognition in support work proceeds otherwise: the practitioner does not list conditions, they pick out the coherence of a pattern through the account, the manner, the details the person sets down over the interview. Operational criterion and clinical recognition operate at two distinct levels and coexist in practice. Establishing the concordance between the operational criterion and a clinical reference standard would be a separate step, which this paper does not anticipate.
Beyond these direct tests, several research directions open up. A psychometric operationalization of the entry marker (defined in §4), the “no” answer to the pivot question, read together with the convergence of the markers (stress that no longer comes down, background anxiety that will not let go), would make it possible to test whether entry into the gray zone can be detected by a short, reproducible instrument. In the absence of a stable biological signature of burnout (Balia et al., 2025, preprint), such a marker would stay phenomenological; experience sampling protocols, which capture the fine-grained dynamics of lived states, offer a methodological precedent (Frick et al., 2024).
A structural limit of any map built from post-T1 clinical work has to be named: the people observed are, by construction, the ones who actually crossed T1. The recurring phrase “I didn’t see it coming” is conditioned on the collapse. The gray zone in fact has several possible exits: a resignation, the end of a project, a decision that loosens the constraint, sick leave for another cause, all trajectories that do not reach T1 and that the retrospective setup does not observe. This double selection (on entering the territory and on exiting through T1) makes it impossible to establish, from these data alone, that the gray zone is specific to the burnout-collapse trajectory. A prospective longitudinal study would make it possible to observe the territory setting in over time, its proximity to T1, and to test whether the duration of SF correlates with the magnitude of the post-collapse toll. Support work proceeds by retrospective reconstruction, where a prospective protocol would reach the forming of the plateau.
Recent clinical literature also recognizes that burnout admits internal heterogeneity: subtypes that partly preserve effectiveness, mild/subclinical subgroups, nonlinear longitudinal trajectories (van Dam, 2016; Bauernhofer et al., 2018; Bondjers et al., 2025); this post-T1 heterogeneity supports the status of the territory described here, to be understood as an entry point common to several possible trajectories rather than a single station on a linear sequence.
Tests on other populations and in other contexts (including outside the work sphere, as the §6 vignette suggests) would probe the reach of the mode: SF is probably not specific to work burnout, but work burnout remains the most institutionally documented occurrence, and so the most accessible entry ground.
10. Summary and conclusion
This paper has set out a territory and how it works. The gray zone is a prodromal plateau, bounded by two thresholds (T0, the switch that opens the crossing; T1, the collapse that closes it) and occupied by a mode of its own: Survival Functioning, which draws on vital reserves to keep up fragments of functioning, sustained by a compensatory loop. Four mechanisms (attentional capture, allostatic recalibration, mislabeling, discounting) make it go unseen, by the person who crosses it as by those around them.
If this territory has stayed nameless, it is not for want of attention. Its illegibility is set out as a configurational property, not an individual failing; it is not resolved by an effort of will or by closer observation.
Validated instruments (BAT, MBI, clinical scales) measure a state at the point of clinical contact, most often at the collapse or after, whereas the crossing plays out before (§1). It is this phase that the mapping seeks to make something you can spot, subject to testing: its entry marker stays phenomenological there, not operationalized, a landmark to test, not an established test. Yet this phase can be described ahead of time. The switch into Survival Functioning is close to an experience everyone has had, that of a wave of fatigue you had to push through by forcing yourself; the grandmother in §6 gives it in its pure form. This is what lets you describe T0 to someone who has not yet crossed it. Placing it in time is another matter: the moment a person crosses T0 is recognized only after the fact (§5), and this paper does not try to detect it. The collapse is a dated event: the reconstruction starts there and works back to T0. T1 thus provides the observable anchor point of the approach; T0 stays a reconstructed landmark. In practice, what matters is not T0 itself, but the signs that follow it.
The professionals who meet these people before T1 (an occupational physician, say) already recognize the signs: the pressure, the constant stress, the inability to switch off, the exhaustion. What they have less readily at hand is the mechanism behind it: why this phase stays illegible, and what locks the person inside it when they feel they have no choice. That is where this framework offers to add something, not on signs already known.
This paper lays out the mapping the way a practitioner formalizes what they have observed: from trajectories reconstructed in support work, cross-checked against what other traditions have described (allostasis, attention, transactional analysis). Each of these traditions describes one piece and documents it in its own field; none, taken alone, produces a T0 or carries the trajectory all the way to collapse. What this paper adds is not one more piece, but their arrangement: the place and role of each in the architecture from which T0, then the crossing through to T1, become intelligible. The approach is abductive; what it produces is a synthesis to be tested, not a closed thesis. What has been drawn from a practice now calls for independent testing: test the entry marker; track over time whether longer Survival Functioning predicts a heavier toll; and test, finally, whether this structure, anchored here on burnout, holds beyond it. The map is on the table, for those who will want to take it further: to adjust it, extend it, or refute it.
Transparency declarations
Document status. This text is published as a preprint, made public for discussion ahead of any formal editorial route through a peer-reviewed journal.
Caution on use. This paper describes a territory and how it works and offers it up for testing; it is not a diagnostic tool and replaces neither medical advice nor validated clinical instruments. A reader who recognizes themselves in the signs described is encouraged to speak to a health professional without delay. The mapping directs attention; it does not make a diagnosis and does not measure a state. The map describes a way of functioning; it does not assign responsibility, and it is not a basis for attributing the collapse to the person or for setting aside what that person reports about their own state.
Illustrative vignette. The “Sarah” case and the grandmother vignette (§6) presented in this paper are composite vignettes built for the purpose of educational illustration. They condense recurring patterns observed in the author’s support practice, correspond to no real person, and draw on no personal data. No biographical detail points to an identifiable clinical case. Accordingly, this work did not require ethics committee review or an individual consent procedure.
Conflicts of interest. The author practices as a certified professional coach (RNCP7, ICN Business School 2019) at Deep Sense Sàrl-S (Luxembourg), where he develops his own practitioner tools, including the MABI (Mputu Advanced Burnout Indicator). Some of these tools draw on elements articulated here. The paper’s conceptual contributions are released under a CC BY 4.0 license, freely reusable including by third parties, with nothing reserved to the author’s activity. Indirect repercussions through a reputation effect on the author’s activity cannot be ruled out.
Funding. This work received no external funding.
Data availability. Not applicable. This paper is a theory synthesis paper (Jaakkola, 2020) that articulates existing theoretical frameworks from recurring patterns observed in the author’s practice. It draws on no empirical data in the quantitative sense (cohort, questionnaire, sample). The practitioner observations it rests on are condensed in the illustrative vignette described above.
Use of artificial intelligence tools. In line with the ICMJE recommendations (2026, Section V.A), the author declares having used a conversational assistant, Claude (Anthropic), as an interlocutor to discuss and refine the presentation of the ideas against academic standards, and as support for formatting, for locating bibliographic anchors, and for translating the text from the original French into English. The conception of the framework, the lived material, the clinical observations, the proposed mapping, the mechanisms described, the propositions offered, and the original French writing fall under the author’s full intellectual responsibility; the English translation was produced with this assistance and reviewed and validated by the author.
Correspondence and collaboration. The author, a practitioner, does not himself undertake the empirical testing of the mapping: he sets it down and welcomes contact from researchers wishing to test it, deepen it, or co-develop it. ORCID: https://orcid.org/0009-0001-2677-9142.
References
Apgar, V. (1953). A proposal for a new method of evaluation of the newborn infant. Current Researches in Anesthesia and Analgesia, 32(4), 260–267.
Arnsten, A. F. T. (2009). Stress signalling pathways that impair prefrontal cortex structure and function. Nature Reviews Neuroscience, 10(6), 410–422. https://doi.org/10.1038/nrn2648
Assurance Maladie – Risques professionnels. (2025). Rapport annuel 2024 de l’Assurance Maladie – Risques professionnels [2024 annual report of the French statutory health insurance – Occupational Risks branch]. Caisse nationale de l’Assurance Maladie. https://www.assurance-maladie.ameli.fr/etudes-et-donnees/2024-rapport-annuel-assurance-maladie-risques-professionnels
Bakker, A. B., & De Vries, J. D. (2021). Job demands–resources theory and self-regulation: New explanations and remedies for job burnout. Anxiety, Stress, & Coping, 34(1), 1–21. https://doi.org/10.1080/10615806.2020.1797695
Balia, M., Zenasni, F., Lepoittevin, M., Bianchi, R., Julian, A., Bodard, S., & Bringer, M. (2025). Toward early detection of burnout: A systematic review of potential biomarkers. medRxiv [Preprint]. https://doi.org/10.1101/2025.08.05.25332953
Bärtl, C., Henze, G.-I., Giglberger, M., Peter, H. L., Konzok, J., Wallner, S., Kreuzpointner, L., Wüst, S., & Kudielka, B. M. (2022). Higher allostatic load in work-related burnout: The Regensburg Burnout Project. Psychoneuroendocrinology, 143, 105853. https://doi.org/10.1016/j.psyneuen.2022.105853
Bauernhofer, K., Bassa, D., Canazei, M., Jiménez, P., Paechter, M., Papousek, I., Fink, A., & Weiss, E. M. (2018). Subtypes in clinical burnout patients enrolled in an employee rehabilitation program. BMC Psychiatry, 18(1), 10. https://doi.org/10.1186/s12888-018-1589-y
Bianchi, R., & Schonfeld, I. S. (2025). Beliefs about burnout. Work & Stress, 39(2), 116–134. https://doi.org/10.1080/02678373.2024.2364590
Bobba-Alves, N., Juster, R.-P., & Picard, M. (2022). The energetic cost of allostasis and allostatic load. Psychoneuroendocrinology, 146, 105951. https://doi.org/10.1016/j.psyneuen.2022.105951
Boksem, M. A. S., & Tops, M. (2008). Mental fatigue: Costs and benefits. Brain Research Reviews, 59(1), 125–139. https://doi.org/10.1016/j.brainresrev.2008.07.001
Bondjers, K., Hyland, P., Atar, D., Christensen, J. O., Nilsen, K. B., Reitan, S. K., Rosseland, L. A., Wentzel-Larsen, T., Wøien, H., Zwart, J. A., Dyb, G., & Stensland, S. (2025). Burnout trajectories among healthcare workers during a pandemic, and predictors of change. BMC Health Services Research, 25(1), 757. https://doi.org/10.1186/s12913-025-12802-w
Borsboom, D., van der Maas, H. L. J., Dalege, J., Kievit, R. A., & Haig, B. D. (2021). Theory construction methodology: A practical framework for building theories in psychology. Perspectives on Psychological Science, 16(4), 756–766. https://doi.org/10.1177/1745691620969647
Brierley, J. D., Gospodarowicz, M. K., & Wittekind, C. (Eds.). (2017). TNM classification of malignant tumours (8th ed.). Wiley Blackwell. [Published in affiliation with the Union for International Cancer Control (UICC).]
Cohen, J. (1960). A coefficient of agreement for nominal scales. Educational and Psychological Measurement, 20(1), 37–46. https://doi.org/10.1177/001316446002000104
Damasio, A. R. (1994). Descartes’ error: Emotion, reason, and the human brain. G. P. Putnam’s Sons.
de Croon, E. M., Sluiter, J. K., & Frings-Dresen, M. H. W. (2003). Need for recovery after work predicts sickness absence: A 2-year prospective cohort study in truck drivers. Journal of Psychosomatic Research, 55(4), 331–339. https://doi.org/10.1016/S0022-3999(02)00630-X
Demerouti, E., & Bakker, A. B. (2025). Revitalising burnout research. Work & Stress, 39(2), 153–161. https://doi.org/10.1080/02678373.2025.2473385
Dettmers, J., Deci, N., Baeriswyl, S., Berset, M., & Krause, A. (2016). Self-endangering work behavior. In M. Wiencke, M. Cacace, & S. Fischer (Eds.), Healthy at work: Interdisciplinary perspectives (pp. 37–51). Springer. https://doi.org/10.1007/978-3-319-32331-2_4
Freudenberger, H. J. (1974). Staff burn-out. Journal of Social Issues, 30(1), 159–165. https://doi.org/10.1111/j.1540-4560.1974.tb00706.x
Frick, S., van der Meij, L., Smolders, K., Demerouti, E., & de Kort, Y. (2024). The effect of time and day of the week on burnout-related experiences: An experience sampling study. European Journal of Work and Organizational Psychology, 33(3), 276–293. https://doi.org/10.1080/1359432X.2023.2266874
Fries, E., Hesse, J., Hellhammer, J., & Hellhammer, D. H. (2005). A new view on hypocortisolism. Psychoneuroendocrinology, 30(10), 1010–1016. https://doi.org/10.1016/j.psyneuen.2005.04.006
Glise, K., Ahlborg, G., Jr., & Jonsdottir, I. H. (2012). Course of mental symptoms in patients with stress-related exhaustion: Does sex or age make a difference? BMC Psychiatry, 12, 18. https://doi.org/10.1186/1471-244X-12-18
Goffman, E. (1959). The presentation of self in everyday life. Doubleday.
Golembiewski, R. T., & Munzenrider, R. F. (1988). Phases of burnout: Developments in concepts and applications. Praeger.
Haig, B. D. (2005). An abductive theory of scientific method. Psychological Methods, 10(4), 371–388. https://doi.org/10.1037/1082-989X.10.4.371
Hallsten, L., Josephson, M., & Torgén, M. (2005). Performance-based self-esteem: A driving force in burnout processes and its assessment (Arbete och Hälsa 2005:4). National Institute for Working Life.
Haute Autorité de Santé. (2017). Repérage et prise en charge cliniques du syndrome d’épuisement professionnel ou burnout [Clinical identification and management of occupational burnout syndrome]. HAS. https://www.has-sante.fr/jcms/c_2769318/fr/reperage-et-prise-en-charge-cliniques-du-syndrome-d-epuisement-professionnel-ou-burnout
Hobfoll, S. E. (1989). Conservation of resources: A new attempt at conceptualizing stress. American Psychologist, 44(3), 513–524. https://doi.org/10.1037/0003-066X.44.3.513
Hochschild, A. R. (1983). The managed heart: Commercialization of human feeling. University of California Press.
Hockey, G. R. J. (1997). Compensatory control in the regulation of human performance under stress and high workload: A cognitive-energetical framework. Biological Psychology, 45(1–3), 73–93. https://doi.org/10.1016/S0301-0511(96)05223-4
International Committee of Medical Journal Editors. (2026). Recommendations for the conduct, reporting, editing, and publication of scholarly work in medical journals. Retrieved June 3, 2026, from https://www.icmje.org/recommendations/
International Labour Organization. (2026). The psychosocial working environment: Global developments and pathways for action. International Labour Office. https://www.ilo.org/publications/psychosocial-working-environment-global-developments-and-pathways-action
Jaakkola, E. (2020). Designing conceptual articles: Four approaches. AMS Review, 10(1–2), 18–26. https://doi.org/10.1007/s13162-020-00161-0
Karakolias, S. (2025). Seeing burnout coming: Early signs and recognition strategies in health professionals. Frontiers in Public Health, 13, 1721220. https://doi.org/10.3389/fpubh.2025.1721220
Karanika-Murray, M., & Biron, C. (2020). The health-performance framework of presenteeism: Towards understanding an adaptive behaviour. Human Relations, 73(2), 242–261. https://doi.org/10.1177/0018726719827081
Kitchener, B. A., Jorm, A. F., & Kelly, C. M. (2015). Mental Health First Aid international manual. Mental Health First Aid International.
Krippendorff, K. (2004). Content analysis: An introduction to its methodology (2nd ed.). Sage.
Kunda, Z. (1990). The case for motivated reasoning. Psychological Bulletin, 108(3), 480–498. https://doi.org/10.1037/0033-2909.108.3.480
Lastovkova, A., Carder, M., Rasmussen, H. M., Sjoberg, L., de Groene, G. J., Sauni, R., Vevoda, J., Vevodova, S., Lasfargues, G., Svartengren, M., Varga, M., Colosio, C., & Pelclova, D. (2018). Burnout syndrome as an occupational disease in the European Union: An exploratory study. Industrial Health, 56(2), 160–165. https://doi.org/10.2486/indhealth.2017-0132
Lazarus, R. S. (1991). Emotion and adaptation. Oxford University Press.
LeDoux, J. E. (1996). The emotional brain: The mysterious underpinnings of emotional life. Simon & Schuster.
Leventhal, H., Meyer, D., & Nerenz, D. R. (1980). The common sense representation of illness danger. In S. Rachman (Ed.), Contributions to medical psychology (Vol. 2, pp. 17–30). Pergamon Press.
Logan, G. D. (1988). Toward an instance theory of automatization. Psychological Review, 95(4), 492–527. https://doi.org/10.1037/0033-295X.95.4.492
Mackie, J. L. (1965). Causes and conditions. American Philosophical Quarterly, 2(4), 245–264.
Maslach, C., Schaufeli, W. B., & Leiter, M. P. (2001). Job burnout. Annual Review of Psychology, 52, 397–422. https://doi.org/10.1146/annurev.psych.52.1.397
McElhinney, Z., & Kennedy, C. (2022). Enhancing the collective, protecting the personal: The valuable role of composite narratives in medical education research. Perspectives on Medical Education, 11(4), 220–227. https://doi.org/10.1007/s40037-022-00723-x
McEwen, B. S. (1998). Protective and damaging effects of stress mediators. New England Journal of Medicine, 338(3), 171–179. https://doi.org/10.1056/NEJM199801153380307
Mellor, K., & Schiff, E. (1975). Discounting. Transactional Analysis Journal, 5(3), 295–302. https://doi.org/10.1177/036215377500500321
Parker, G., & Russo, N. (2025). Current issues in relation to burnout’s definition, measurement, prevalence and management: A narrative review. Psychiatry Research, 352, 116709. https://doi.org/10.1016/j.psychres.2025.116709
Pauly, D. (1995). Anecdotes and the shifting baseline syndrome of fisheries. Trends in Ecology & Evolution, 10(10), 430. https://doi.org/10.1016/S0169-5347(00)89171-5
Pennebaker, J. W. (1982). The psychology of physical symptoms. Springer-Verlag. https://doi.org/10.1007/978-1-4613-8196-9
Petriglieri, J. L. (2011). Under threat: Responses to and the consequences of threats to individuals’ identities. Academy of Management Review, 36(4), 641–662. https://doi.org/10.5465/amr.2009.0087
Rotenstein, L. S., Torre, M., Ramos, M. A., Rosales, R. C., Guille, C., Sen, S., & Mata, D. A. (2018). Prevalence of burnout among physicians: A systematic review. JAMA, 320(11), 1131–1150. https://doi.org/10.1001/jama.2018.12777
Salmela-Aro, K., Hietajärvi, L., & Lonka, K. (2019). Work burnout and engagement profiles among teachers. Frontiers in Psychology, 10, 2254. https://doi.org/10.3389/fpsyg.2019.02254
Schaufeli, W. B., De Witte, H., Hakanen, J. J., Kaltiainen, J., & Kok, R. (2023). How to assess severe burnout? Cutoff points for the Burnout Assessment Tool (BAT) based on three European samples. Scandinavian Journal of Work, Environment & Health, 49(4), 293–302. https://doi.org/10.5271/sjweh.4093
Schaufeli, W. B., Desart, S., & De Witte, H. (2020). Burnout Assessment Tool (BAT) — Development, validity, and reliability. International Journal of Environmental Research and Public Health, 17(24), 9495. https://doi.org/10.3390/ijerph17249495
Schön, D. A. (1983). The reflective practitioner: How professionals think in action. Basic Books.
Schooler, J. W. (2002). Re-representing consciousness: Dissociations between experience and meta-consciousness. Trends in Cognitive Sciences, 6(8), 339–344. https://doi.org/10.1016/S1364-6613(02)01949-6
Schulz, A., & Vögele, C. (2015). Interoception and stress. Frontiers in Psychology, 6, 993. https://doi.org/10.3389/fpsyg.2015.00993
Schwabe, L., & Wolf, O. T. (2009). Stress prompts habit behavior in humans. Journal of Neuroscience, 29(22), 7191–7198. https://doi.org/10.1523/JNEUROSCI.0979-09.2009
Scott, S. E., Walter, F. M., Webster, A., Sutton, S., & Emery, J. (2013). The Model of Pathways to Treatment: Conceptualization and integration with existing theory. British Journal of Health Psychology, 18(1), 45–65. https://doi.org/10.1111/j.2044-8287.2012.02077.x
Shah, J. Y., Friedman, R., & Kruglanski, A. W. (2002). Forgetting all else: On the antecedents and consequences of goal shielding. Journal of Personality and Social Psychology, 83(6), 1261–1280. https://doi.org/10.1037/0022-3514.83.6.1261
Siegrist, J. (1996). Adverse health effects of high-effort/low-reward conditions. Journal of Occupational Health Psychology, 1(1), 27–41. https://doi.org/10.1037/1076-8998.1.1.27
Smeets, T., Ashton, S. M., Roelands, S. J. A. A., & Quaedflieg, C. W. E. M. (2023). Does stress consistently favor habits over goal-directed behaviors? Data from two preregistered exact replication studies. Neurobiology of Stress, 23, 100528. https://doi.org/10.1016/j.ynstr.2023.100528
Socialstyrelsen. (2003). Utmattningssyndrom: Stressrelaterad psykisk ohälsa [Exhaustion disorder: Stress-related mental ill-health] (Artikelnummer 2003-123-18). https://www.socialstyrelsen.se/publikationer/utmattningssyndrom--stressrelaterad-psykisk-ohalsa-2003-123-18/
Soga, M., & Gaston, K. J. (2024). Global synthesis indicates widespread occurrence of shifting baseline syndrome. BioScience, 74(10), 686–694. https://doi.org/10.1093/biosci/biae068
Spielman, A. J., Caruso, L. S., & Glovinsky, P. B. (1987). A behavioral perspective on insomnia treatment. Psychiatric Clinics of North America, 10(4), 541–553.
Steptoe, A., & Marmot, M. (2005). Impaired cardiovascular recovery following stress predicts 3-year increases in blood pressure. Journal of Hypertension, 23(3), 529–536. https://doi.org/10.1097/01.hjh.0000160208.66405.a8
Sterling, P., & Eyer, J. (1988). Allostasis: A new paradigm to explain arousal pathology. In S. Fisher & J. Reason (Eds.), Handbook of life stress, cognition and health (pp. 629–649). John Wiley & Sons.
Teasdale, G., & Jennett, B. (1974). Assessment of coma and impaired consciousness: A practical scale. The Lancet, 304(7872), 81–84. https://doi.org/10.1016/S0140-6736(74)91639-0
van Dam, A. (2016). Subgroup analysis in burnout: Relations between fatigue, anxiety, and depression. Frontiers in Psychology, 7, 90. https://doi.org/10.3389/fpsyg.2016.00090
van Dam, A. (2021). A clinical perspective on burnout: Diagnosis, classification, and treatment of clinical burnout. European Journal of Work and Organizational Psychology, 30(5), 732–741. https://doi.org/10.1080/1359432X.2021.1948400
Van de Ven, A. H. (2007). Engaged scholarship: A guide for organizational and social research. Oxford University Press.
Vandenabeele, R., Joosen, M. C. W., & van Dam, A. (2025). Chronic stress in relation to clinical burnout: An integrative scoping review of definitions and measurement approaches. Frontiers in Psychology, 16, 1712340. https://doi.org/10.3389/fpsyg.2025.1712340
Whitaker, K. L., Scott, S. E., & Wardle, J. (2015). Applying symptom appraisal models to understand sociodemographic differences in responses to possible cancer symptoms: A research agenda. British Journal of Cancer, 112(Suppl 1), S27–S34. https://doi.org/10.1038/bjc.2015.39
Willis, R. (2019). The use of composite narratives to present interview findings. Qualitative Research, 19(4), 471–480. https://doi.org/10.1177/1468794118787711
World Health Organization. (2019, May 28). Burn-out an “occupational phenomenon”: International Classification of Diseases [News release]. https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases
Yung, A. R., & McGorry, P. D. (1996). The prodromal phase of first-episode psychosis: Past and current co